



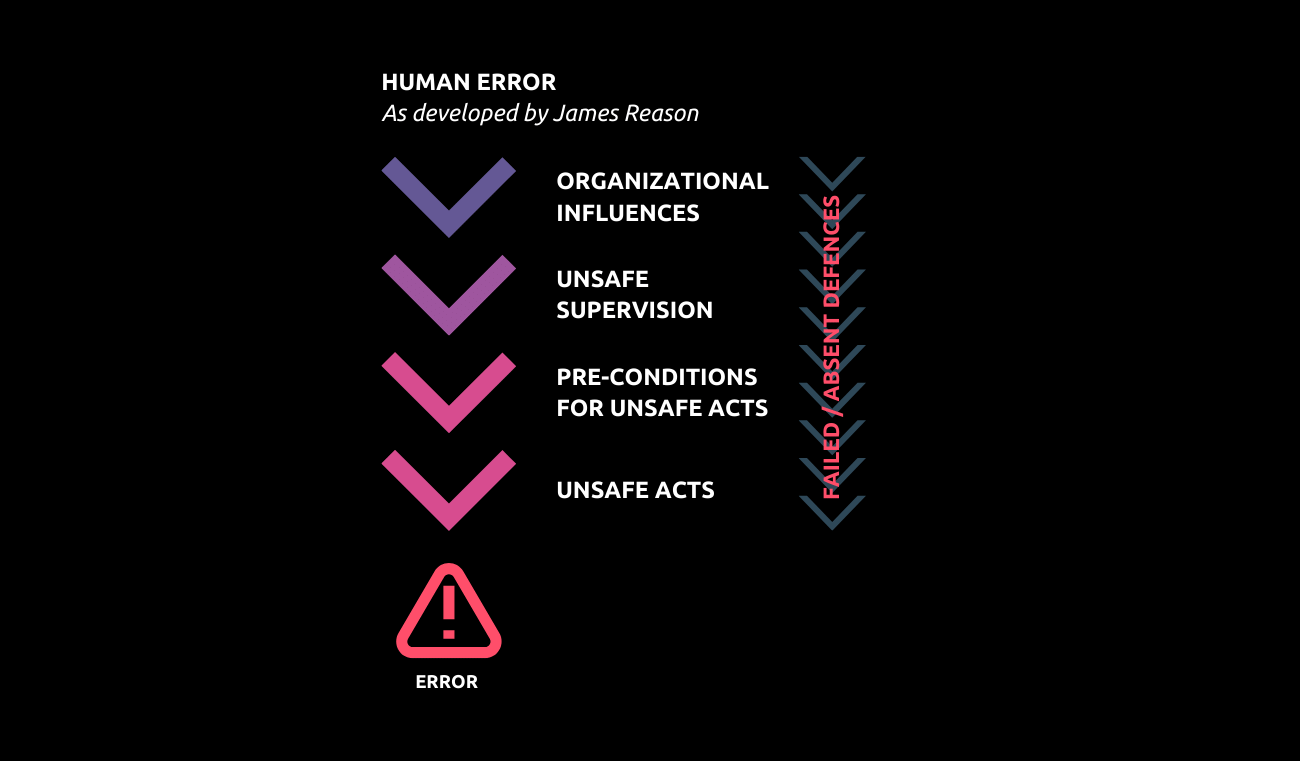
Human Factors in Patient Safety
Read as Magazine PDF
What impacts occur and what solutions exist concerning human factors?
HISTORY:
1980’s: CQI (Continuous Quality Improvement)
1990’s: Complaints and Litigation
1999: National Adverse Event Studies, Reporting systems, AE analysis
2000: Prescriptive Vision of Safety – Safety is following the rule, Evidence-based Medicine, and a search for compliance
This led to a systemic migration to boundaries.
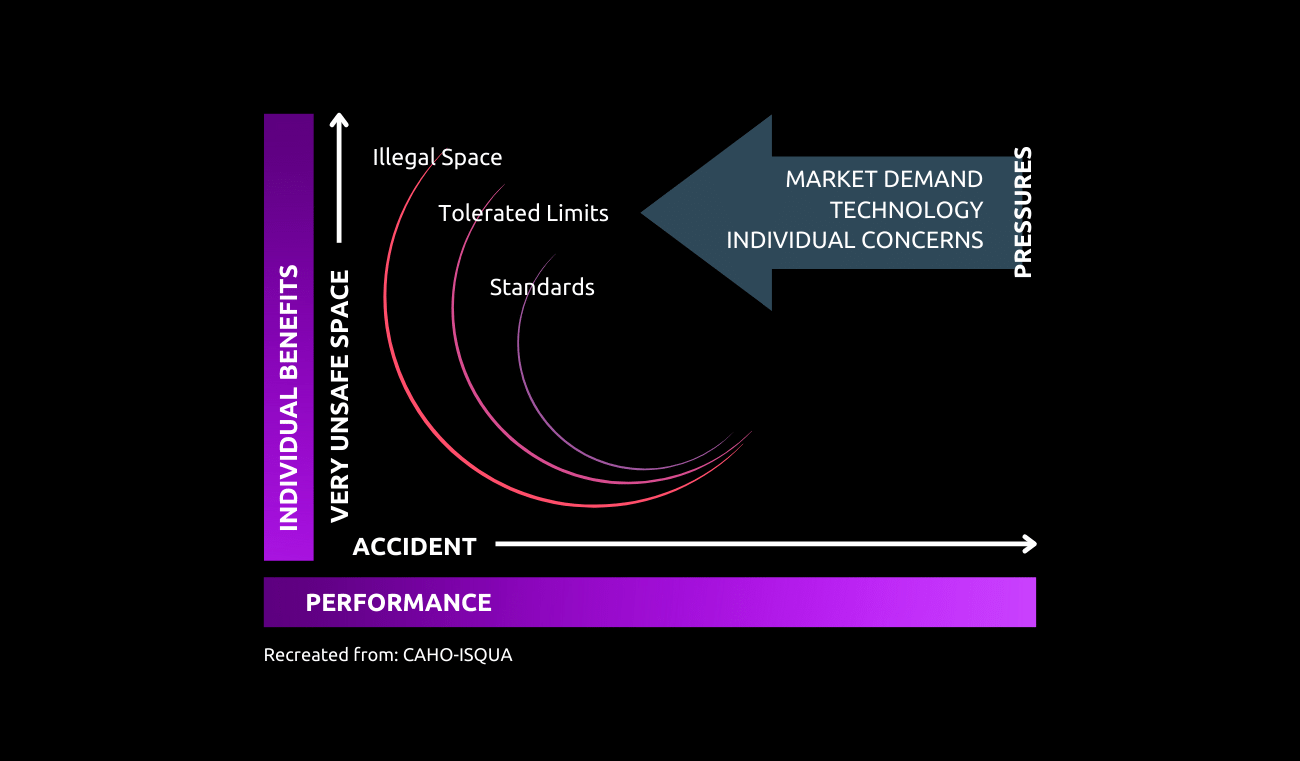
When you are designing a system, you have the market demand, the technology, and the individual concerns, and you are designing an expected safe space of action as defined by professional standards, and by quality. And this is the area where you expect the system will work. Always, always.
But the reality is that the performance needed for fulfilling the demand will rapidly push the system towards more performance. And the idea of human factors at that stage was to maintain the system as far as possible from the red line, where the system begins to be unsafe.
The reality is probably more difficult because very quickly in our systems you have a migration that makes acute borderline tolerated conditions of using a normal in the system. If you have one nurse missing or one doctor missing, you will never stop working in a hospital because you have one nurse missing or one doctor missing. The system compensates by being on the borderline until practices in this borderline situation become normalized by human factors. So staff shortage is a good example of a system which migrates very quickly out of what was expected by the regulation, or at least by the standards.
And this is one of the reasons why the system is progressively moving towards the red. The very problem is how to contain this move because once you are in this usual space of action with accepted tolerances, the people working in this area like the nurses, for example, are working every day in conditions of staff shortage. They will also take benefit from that and will reorganize their planning in conditions where it is not needed just because it is something that the administration has accepted as use or space of action. So in the end, it is creating a system which is outside the normal condition. And this is very normal for our healthcare system at present.
We should prevent it from deteriorating further and entering even illegal territory. And the very problem of this move with the system is that what you expected becomes something that generally stays as only a paper and pencil exercise. And the reality on the ground makes the authority themselves, the hierarchy, and the management chain see that they have moved to something that is borderline – the tolerated condition of use.
- 2005 – 2010: Safer drug management initiatives
- 2009: WHO Surgical Safety Checklist
- 2005-2015: Safer communication, teamwork and coordination
Most of these adaptations have been from taking lessons from other industries. The need for recovering from work and fatigue among physicians was also adopted from the aviation industry along with checklists. The idea of effective safety culture was imported from other industries as well.
Around 2015, we realized patient safety is becoming more complex as we tackle a rapid change in the issues and complexity of the healthcare system.
- Healthcare systems are transforming at unprecedented levels – In less than 20 years, the world’s population has climbed from 6 to 7.78 billion (+25%). Nearly 20% of additional patients – are more chronic, and more fragile.
- Hospitals and Healthcare Systems have not changed at the same speed. The knowledge and technology of care have changed at a high speed but not the task force and human resources.
- Signs of Progress are made at zero cost – With the imperative of changing and changing again for reallocating means, resources and finances. The GDP per capita for medical affairs cannot change that much since it was already high before the last revolution
- Medical workers are affected by these revolutions, continuously being pushed to adapt.
- It poses a greater challenge for quality and safety since these dimensions allow only change for the better and do not allow for compromise or adaptation.
The Key Changes from 2015:
- A cascade effect on the conceptual approach to Quality and Safety
- The need to move from a primarily event-focussed acute system to a longitudinal life-course perspective
- Profound consequences on how we conceptualize safety and quality and re-prioritize human factors
- Safety is no longer described in terms of episodic risk suppression but in terms of controlling acceptable risk over time in both the short and the long term
- Solutions for optimizing Quality & Medical efficiency (proposing the best of medical knowledge) are not equal to solutions optimizing Safety (controlling risks in a greater variety of medical settings, including small isolated hospitals, home care and community care.
- A need to re-conceptualize the very nature and use of Quality and Safety standards of the 21st century, their interpretation and role in system changes and progress, and all related human factor priorities.
The half-life of medical knowledge now is below 6 years in most specialities, it is 17 years for nuclear, and 13 years for aviation. The closest is the software industry at 2.6 years.
The Move to Patient Journey
Change in time scale: We no longer focus on a specific part of the care like primary care. We envision the whole process from the start to the end of care for the patient.
A New Focus:
- The transition of Care: How care is being delivered in various environments the patient navigates during the course of the illness from home to the different departments and back to home, perhaps. The way we are passing the information and coordinating all carers in the patient journey in time scales than may span years is a view we are slowly beginning to take
- Primary care & Homecare: Focus on these areas apart from improving safety in hospitals alone
- Adopt a system vision: This 360-degree focus is ensuring that we see the whole system together while planning and implementing changes.
Safety in healthcare is a moving target
- Profound consequences on how we conceptualize safety and quality and re-prioritize human factors
- Safety is no longer described in terms of episodic risk suppression but in terms of controlling acceptable risk over time in both the short and the long term
- Solutions for optimizing Quality & Medical efficiency (proposing the best of medical knowledge) are not equal to solutions for optimizing Safety (controlling risks in a greater variety of medical settings, including small isolated hospitals, home care and community care.
- A need to re-conceptualize the very nature and use of Quality and Safety standards of the 21st century, their interpretation and role in system changes and progress, and all related human factor priorities.
- The half-life of medical knowledge now is below 6 years in most specialities, it is 17 years for nuclear, and 13 years for aviation. The closest is the software industry at 2.6 years.
The Move to Patient Journey
- Change in time scale: We no longer focus on a specific part of the care like primary care. We envision the whole process from the start to the end of care for the patient.
- New Focus:
- The transition of Care: How care is being delivered in various environments the patient navigates during the course of the illness from home to the different departments and back to home, perhaps. The way we are passing the information and coordinating all carers in the patient journey in time scales than may span years is a view we are slowly beginning to take
- Primary care & Homecare: Focus on these areas apart from improving safety in hospitals alone
- Adopt a system vision: This 360-degree focus is ensuring that we see the whole system together while planning and implementing changes.
- Poor access – This has moved from accessibility based on money to accessibility to the right specialists and carers and the dimension of the problem has shifted.
- Adverse events associated with poor care
- Adverse events associated with the care environment
- Poor shared information and partnership with patients – This is a target that has become highlighted only recently. Patients need information that makes sense and takes a view of their health from a long-term perspective.
- Incredible errors/ Never events
Since the targets themselves are evolving, we can not even measure our progress properly unlike in other industries and this presents healthcare with a unique problem.
CHRONIC STAFF SHORTAGE IMPACTS CHRONIC ORGANIZATIONAL FACTORS
- Working under staff and material constraints are becoming the norm around the world with few exceptions
- The lack of personnel accelerates fatigue, disrupts teamwork, and concentrates the care on its technical aspect, to other detriments of the more global care of a person
- The COVID crisis further aggravated the problem
WHAT IMPACT OCCURS AND WHAT SOLUTIONS CAN BE IMPLEMENTED ABOUT HUMAN FACTORS?
Challenges:
- We know the building blocks of human factors and patient safety rather well and now we have to learn to use them to ride the horse in the storm of challenging circumstances
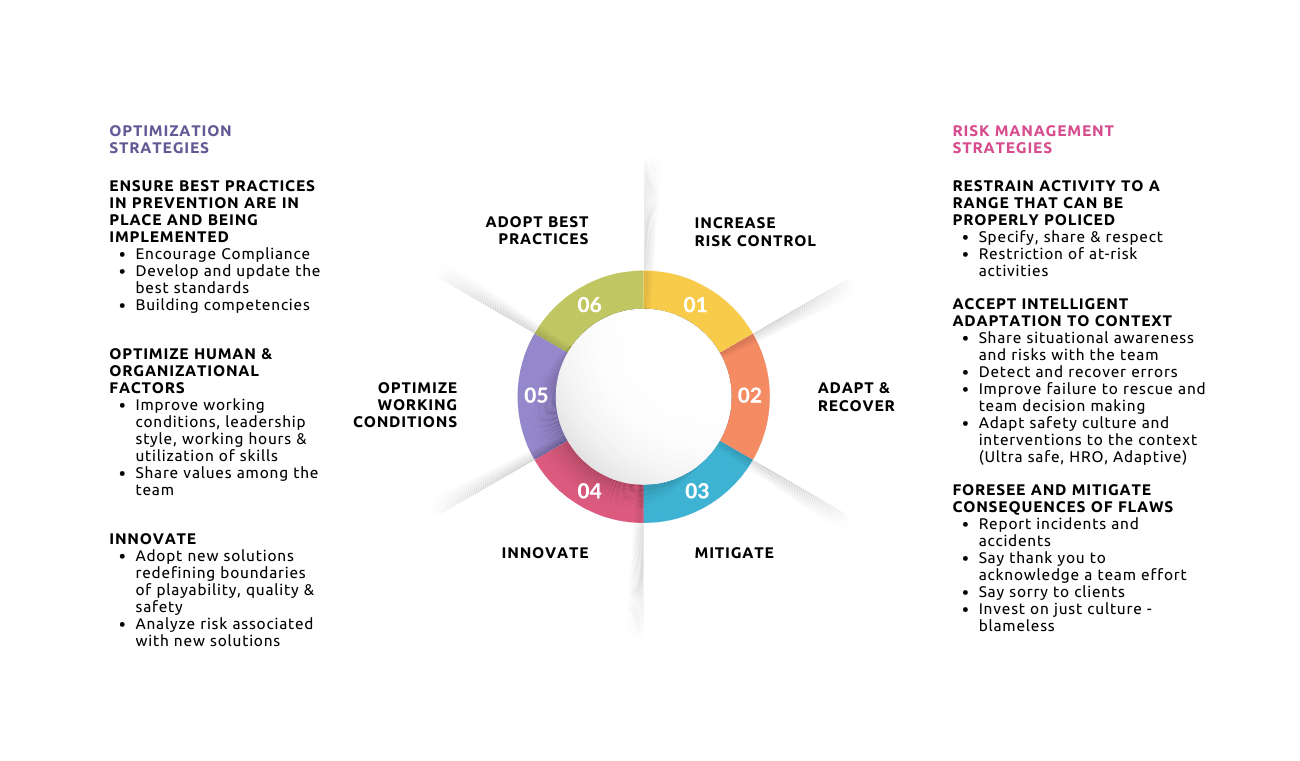
- We are constantly facing a diverging problem. One side accelerating towards optimized adaptation through a consistently high demand for medical care as well as its quality. The other side is optimized adaptability where we must maintain our ability to be dynamic in addressing evolving problems. This requires giving more freedom to people to go beyond accepted methods
- Escaping excessive and radical simplification in the opposition of solutions and managing a balance between the opposing visions of optimizing science patient results and cost-effectiveness and of optimizing worker and system adaptability to a wide variety of contexts.
We cannot continue with a conflict of vision. We need to try to find a tentative solution for encompassing both ideas. We need to continue developing better strategies at an affordable cost for taking care of patients. That’s the job of health care and that we need to deliver.
We are in this for the long haul and we can not expect optimal solutions to existing for the next few decades.
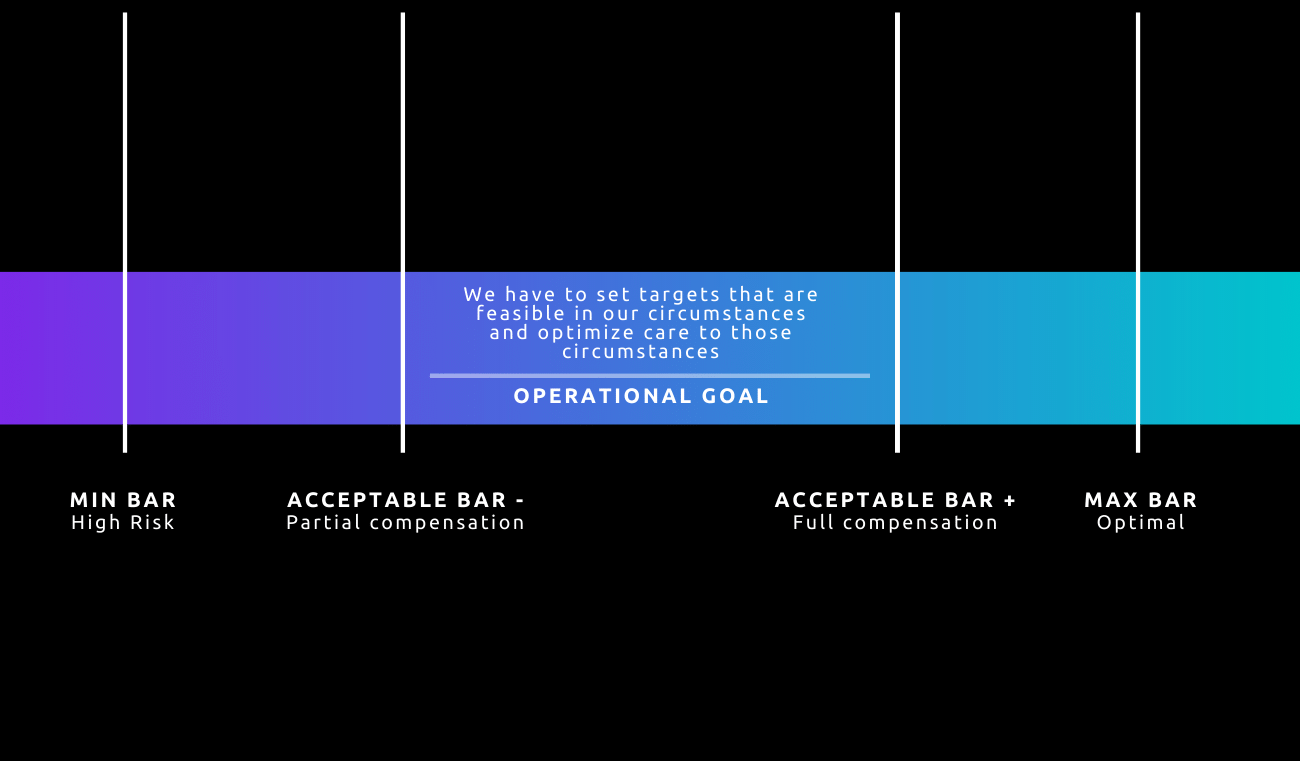
It’s also very important that the conditions that we describe at the ideal level are not feasible at the local level in 80% of the hospitals and medical settings. So we need both. We need to optimize adaptation for the patient, and that demands adaptability for the professionals. Of course, one is more long-term.
When we are working with an accreditation agency and visit a hospital which is not complying totally with the recommendation, we are not closing it. We are giving time. But the idea of giving time to return to normal is to return to the ideal.
HUMAN FACTORS ARE KEY TO REMAINING SAFE ENOUGH WHILE ADAPTING TO A LARGE VARIETY OF CONTEXTS
We are in this for the long haul and we can not expect optimal solutions to exist for the next few decades. We must address key areas of human factors while adapting to these shortcomings.
FRONTLINE MANAGEMENT
- Short briefings, huddles at shift handovers, and anytime the context changes.
- Leadership & Teamwork
- Alerting process
- Values discussion & dialogue
- Enhanced error detection and recovery
- Learning attitude, moments for day’s lessons
- Values celebration, recognition of workers, photos & service recognition
MIDDLE MANAGEMENT
- Planning of work with an honest and relevant analysis of the patient’s specs
- A permanent fight against organizational silence
- Willingness to shorten as much as possible abnormal situations and their causes
- “Moments” dialogues are organized on real working conditions
- A permanent dialogue on autonomy, trust and limitation of trust of frontline managers
- Moments of celebration of good results and safe work
KEY SUMMARY
There is a non-end pressure to improve safety, but:
- The ecosystem largely “directs” the way of working: local, time & financial constraints, hazards etc.
- It is sometimes necessary to navigate across safety models to adapt best to local contexts
- “Work as imagined needs to be designed with a rile-based strategy although accepting that hazards could lead front-line managers punctually adopting a more managed-based strategy
- Navigating towards a more managed-based strategy is not at all easy or intuitive. It must be taught to managers.
- The more the usual model is based on expertise and managed-based safety, the more the need for a strong safety culture
Author
-

Senior Advisor (Patient Safety), Haute Autorite de Sante (HAS), France